Top > About Us > News Letter > Light as a Reliable Guide for Surgery
Light as a Reliable Guide for Surgery: Development of Hepatobiliary and Pancreatic Surgical Operation Using Fluorescence Imaging
From The University of Tokyo Hospital to the World
Hepatobiliary and Pancreatic Surgery / Artificial Organ and Transplantation Surgery Department
Kiyoshi Hasegawa, Professor and Chairman
1: Introduction
Textbooks of anatomy contain illustrations with fat removed and blood vessels colored in red and blue. What if cancers and vessels behind tissues could be visualized during surgical operations, thus enabling more reliable surgeries to be performed? This possibility motivated us to develop the technique of intraoperative fluorescence imaging. Our department has developed fluorescence imaging of the bile duct, liver tumors, and hepatic segments, and proactively applied this procedure to surgical operations since 2007.
2: Development of fluorescence cholangiography
Indocyanine green (ICG) is an agent that has primarily been used for liver functional tests. In the 1960s, ICG was already known to emit fluorescence peaking at approx. 840 nm when ICG bonded to protein was radiated with near infrared rays. We focused on this property and developed the technology known as fluorescence cholangiography, which enables visualization of the structure of the bile duct using light by directly injecting ICG into the bile duct, or by utilizing ICG that is excreted into bile after intravenous injection. [1] This technology has drawn particular attention for its effect of avoiding damaging the bile duct during laparoscopic cholecystectomy, one of the most commonly undertaken surgical procedures for gallstones and gallbladder polyps [2], and has been increasingly used in the U.S., Europe, and other regions.
3: Technology that enables liver cancer to emit light
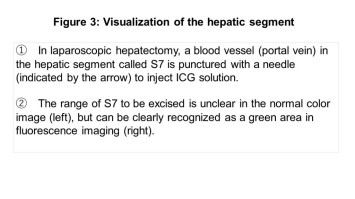
In 2007, when our department was developing fluorescent cholangiography, we found that in addition to the bile duct, cancer tissue in the liver emitted intense fluorescence. [3] Our continued research uncovered the mechanism for this phenomenon, namely that ICG had accumulated inside and/or around the liver cancer following intravenous injection for preoperative liver function tests. [4] By applying this phenomenon to intraoperative imaging, it became possible to identify the location of tumors to be excised using light as a guide. Particularly during laparoscopic hepatectomy, a procedure proactively performed in our department in which an endoscope and rod instruments are inserted and removed through five or six holes in the abdomen, it is not possible for surgeons to confirm the presence of a tumor by directly touching the surface of liver, and therefore, this technology, which localizes cancer based on light emission, is useful to conduct rapid and reliable hepatectomies. [5]
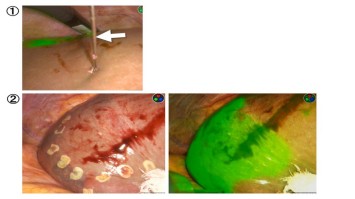
4: Visualization of hepatic segments using light
In surgical operations to remove a liver tumor, it is important to completely excise the entire hepatic segment in which cancer is located rather than only scooping out the primary cancer, in order to avoid leaving behind micro cancerous tissues that expand around the primary cancer. Our department devises an accurate hepatectomy that matches the preoperative plan by distributing ICG throughout the hepatic segment to be excised (or the surrounding segments), and clearly visualizing the borders between the hepatic segments using fluorescence imaging. [6]
5: Efforts toward further enhancing the safety of pancreatectomy
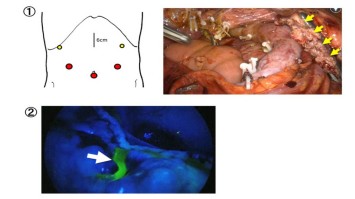
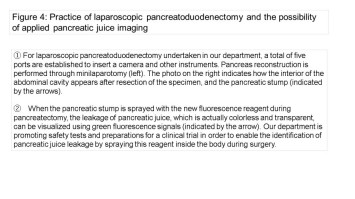
In April 2016, laparoscopic pancreatectomy was included in the scope of insurance coverage. This procedure enables pancreatic surgeries that are usually complicated and involve high postoperative risks with only small surgical wounds. However, no effective solution has been established to prevent pancreatic fistula, the most critical complication associated with pancreatectomy, in which pancreatic juice leaks from the pancreatic stump and/or anastomotic part, resulting in severe damage to patient tissues. Our department is making continuous efforts to further enhance the safety of pancreatic surgery by applying ICG-based fluorescence imaging to the evaluation of organ blood flow around the pancreas, and by also developing a new fluorescence reagent to make pancreatic juice, which is normally colorless and transparent, emit light during surgery. [7]
6: Conclusion
In recent years, the development and clinical application of intraoperative fluorescence imaging has rapidly expanded. Last year, the Japanese Society for Fluorescence Guided Surgery (http://plaza.umin.ac.jp/jsfgs/index.html) (Japanese pages only) was established to provide a forum for information exchange across disciplinary borders. As the secretariat for JSFGS, our department undertakes continuous activities to promote information sharing among surgeons, researchers, and engineers.
1. Ishizawa T, et al. J Am Coll Surg 2008;208:e1-4.
2. Ishizawa T, et al. Br J Surg. 2010;97:1369-77.
3. Ishizawa T, et al. Cancer 2009;115:2491-504.
4. Ishizawa T, et al. Ann Surg Oncol 2014;21:440-8.
5. Kudo H, et al. Surg Endosc 2014;28:2504-81.
6. Yamashita S, et al. Br J Surg 2013;100:1220-8.
7. Miyata A, et al. J Am Coll Surg 2015;221:e27-36.
Departments/Divisions
Pediatrics, Children's Medical Center
Titles
M.D. , Ph.D.
Expertise/Specialties
Pediatrics, Child Neurology, Perinatal and Neonatal Medicine
Research Interests
1) Perinatal brain injury 2) Environmental effects of development
3) Congenital cytomegalovirus infection 4) Developmental disorders
5) Subacute Sclerosing Panencephalitis 6) Public health screening system
Languages
Japanese/ English
See More
Departments/Divisions
Urology and Andrology
Titles
M.D. , Ph.D.
Expertise/Specialties
Robotic Surgery, Laparoscopic Surgery, Endoscopic Surgery, Kidney Cancer, Urinary Tract Cancer, Bladder Cancer, Prostate Cancer, Testicular Cancer, Adrenal Tumor, Renal failure, Peritoneal Dialysis
Research Interests
Molecular Biology, Genome Research
Languages
See More
Departments/Divisions
Clinical Research Governance
Titles
Ph.D.
Expertise/Specialties
Clinical Reseach, GCP, regulation
Research Interests
Quality Management
Languages
Japanese / English
See More
Departments/Divisions
Department of Neurosurgery
Titles
M.D. , Ph.D.
Expertise/Specialties
Acoustic neuroma surgery, Arteriovenous malformation surgery, Skull base meningioma surgery, vertebrobasilar aneurysm surgery
Research Interests
Functional preservation of brain, brainstem and cranial nerves, surgical simulation with 3DCG, functional restoration by brain-machine interface (BMI), neural regeneration by recruitment of endogenous progenitors
Languages
Japanese/ English
See More
Departments/Divisions
Pharmaceutical Department
Titles
Ph.D.
Expertise/Specialties
pharmacy
Research Interests
clinical and molecular pharmacology / toxicology, and systems-biology / pharmacology / toxicology
Languages
Japanese / English
See More
Departments/Divisions
Department of Blood Transfusion
Titles
M.D., Ph.D.
Expertise/Specialties
Transfusion Medicine, Respiratory Medicine, Allergy and Clinical Immunology
Research Interests
Mechanism of transfusion complications, Haemovigilance
Languages
Japanese / English
See More
Departments/Divisions
Department of Pediatric Surgery
Titles
M.D. , Ph.D.
Expertise/Specialties
Pediatric Surgery, Pediatric Minimally Invasive Surgery, Pediatric Oncology, Pediatric Urology, Pediatric HBP Surgery
Research Interests
Pediatric Hepatobiliary disease, Pediatric MIS, Transplantation Immunology
Languages
Japanese/English
See More
Departments/Divisions
Central Supply Service
Titles
M.D. , Ph.D.
Expertise/Specialties
General Surgery, Operative Medicine, Nutrition Support
Research Interests
Surgical Nutrition and Metabolism, Gut Immunity
Languages
Japanese, English
See More
Departments/Divisions
Department of Gastroenterology; Department of Endoscopy and Endoscopic Surgery
Titles
M.D. , Ph.D.
Expertise/Specialties
Gastroenterology, Hepatology (Hepatitis, Hepatocellular Carcinoma), Pancreatology
Research Interests
Viral hepatitis, Hepatocarcinogenesis, NASH, Oxidative stress
Languages
Japanese / English
See More
Departments/Divisions
Allergy and Rheumatology
Titles
M.D. , Ph.D.
Expertise/Specialties
Rheumatology, Internal Medicine
Research Interests
Clinical Immunology, Basic Immunology
Languages
Japanese, English
See More
Departments/Divisions
Department of Psychosomatic Medicine
Titles
M.D. , Ph.D.
Expertise/Specialties
Psychosomatic Medicine
Research Interests
Research on development of treatment for eating disorders and on development of mobile tools for assessment and treatment for life-style related disorders and mood disorders using EMA and EMI methods.
Languages
Japanese / English
See More
Departments/Divisions
Neuropsychiatry, Medical Community Network and Discharge Planning
Titles
M.D. , Ph.D.
Expertise/Specialties
Clinical Psychiatry, Early intervention and rehabilitation for schizophrenia, Community mental health
Research Interests
Neuroimaging in psychiatric disorders, Mental health and neuroscience in adolescence
Languages
Japanese / English
See More
Departments/Divisions
Infection Control and Prevention Service/Department of Infection Control and Prevention Graduate School of Medicine
Titles
M.D. , Ph.D.
Expertise/Specialties
Infection Control and Prevention Service/ Hepatocellular carcinoma, Liver diseases, Viral hepatitis, Liver diseases
Research Interests
Mechanism of hepatocarcinogenesis and relarion between carcinogenesis and mitochondria damage
Languages
Japanese/English
See More
Departments/Divisions
Ophthalmology
Titles
M.D., Ph.D
Expertise/Specialties
Glaucoma, Neurobiochemistry, Ocular Pharmacology
Research Interests
・the analysis of the risk factor activating glaucoma
・the study of the surgical outcomes of glaucoma
・the elucidation to the pathology of increasing intraocular pressure through bioactive lipids
・the development of new drops for glaucoma
Languages
Japanese, English
See More
Departments/Divisions
Breast and Endocrine Surgery
Titles
M.D. , Ph.D.
Expertise/Specialties
surgery on primary breast cancer, systemic treatment on metastatic breast cancer
Research Interests
epigenetic change which is critical for breast cancer development, transcriptional regulation of estrogen receptor alpha (ERα)in breast cancer
Languages
Japanese/English
See More
Departments/Divisions
Division of Nephrology and Endocrinology, Department of Hemodialysis and Apheresis
Titles
M.D. , Ph.D.
Expertise/Specialties
Chronic kidney disease, Acute kidney injury, End stage kidney disesae, Hemodialysis, Nephrotic syndrome, Renal anemia, Atypical hemolytic uremic syndrome
Research Interests
Oxygen metabolism of the kidney, immunological kidney injury, epigenetics, renal anemia
Languages
Japanese/English
See More
Departments/Divisions
Department of Pain and Palliative Medicine
Titles
M.D. , Ph.D.
Expertise/Specialties
Pain Medicine, Palliative Medicine, Anesthesiology, Critical Care Medicine, Medical Engineering
Research Interests
Pain Medicine, Palliative Medicine, Cognitive Neuroscience, Health Literacy
Languages
Japanese
See More
Departments/Divisions
Geriatric Medicine
Titles
M.D. , Ph.D.
Expertise/Specialties
geriatric medicine, gerontology
Research Interests
Pharmacotherapy and its safety in the elderly. Gender difference in geriatric medicine.
Languages
Japanese, English
See More
Departments/Divisions
Department of Hematology and Oncology
Titles
M.D. , Ph.D.
Expertise/Specialties
Hematological malignancies
Research Interests
Leukemia
Languages
Japanese, English
See More
Departments/Divisions
Department of Cardiovascular Surgery & Department of Cooperative Unit of Medicine and Engineering Research
Titles
M.D. , Ph.D.
Expertise/Specialties
Adult Cardiac Surgery, Minimally Invasive Cardiac Surgery, Robotic Cardiac Surgery, Mitral Valve Plasty, Off-pump Coronary Artgery Bypass Surgery, Ventricular Assist Device, Heart Transplantation
Research Interests
Surgical Treatment of End-stage Heart Failure (Ventricular assist device, Heart transplantation, Mitral complex plasty), Device Development for Minimally Invasive Surgery, Regenerative Medicine
Languages
Japanese/English
See More
Departments/Divisions
Plastic Reconstructive and Aesthetic Surgery
Titles
M.D., Ph.D.
Expertise/Specialties
Reanimation of Established Facial paralysis, Reconstruction of Facial Deforimites, Wound Healing
Research Interests
Microsurgery, Facial Paralysis, Ageing
Languages
Japanese/English
See More
Departments/Divisions
Department of Acute Medicine
Critical Care and Emergency Medical Center/Emergency Room, Intensive Care Unit
Titles
M.D., Ph.D
Expertise/Specialties
emergency medicine, critical care medicine, intensive care medicine, disaster medicine, mass gathering medicine
Research Interests
acuity, triage, monitoring, emergency medical service system, disaster medical response system
Languages
English /Japanese
See More
Departments/Divisions
Department of Rehabilitation Medicine, Rehabilitation Center
Titles
M.D. , Ph.D.
Expertise/Specialties
Pediatric Rehabilitation, Rehabilitation and Prosthetics/Orthotics for Congenital Limb Malformation, Rehabilitation for Bone Dysplasias
Research Interests
Pediatric Rehabilitation, Rehabilitation for Disabled Children, Motion Analysis
Languages
Japanese / English
See More
Departments/Divisions
Center for Epidemiology and Preventive Medicine
Titles
M.D. , Ph.D.
Expertise/Specialties
Gastroenterology, Preventive Medicine
Research Interests
Oncology, Epigenetics, Molecular biology, Differentiation and Cancer
Languages
Japanese, English
See More
Departments/Divisions
Neurosurgery
Titles
M.D. , Ph.D.
Expertise/Specialties
Neurosurgery
Research Interests
Surgery of cerebrovascular diseases, Surgery of benign brain tumors, Experimental cerebral ischemia
Languages
Japanese/English
See More
Departments/Divisions
Department of Radiology
Division of Diagnostic Radiology
Titles
M.D., Ph.D
Expertise/Specialties
General diagnostic radiology, neuroradiology, interventional radiology
Research Interests
Voxel-based analysis, voxel-based morphometry, diffusion magnetic resonance imaging,
functional magnetic resonance imaging
Languages
Japanese/English
See More
Departments/Divisions
Stomach and Esophageal Surgery, Cancer Resource Center
Titles
M.D. , Ph.D.
Expertise/Specialties
Abdominal Surgery, General Surgery, Cancer Patients' Care
Research Interests
Gastric Carcinogenesis, Stem Cell and Carcinogenesis, Cancer Biomarker, Cancer Immunology, Growth Factor, Development
Languages
English, Japanese
See More
Departments/Divisions
Orthopaedic Surgery and Spinal Surgery
Titles
M.D. , Ph.D.
Expertise/Specialties
Joint surgery, rheumatoid arthritis, osteoporosis
Research Interests
Bone and cartilage biology, arthritis
Languages
Japanese, English
See More
Departments/Divisions
Dermatology
Titles
M.D. , Ph.D.
Expertise/Specialties
Scleroderma
Research Interests
Scleroderma, B lymphocytes, Autoimmunity
Languages
Japanese/English
See More
Departments/Divisions
Colorectal Surgery; Vascular Surgery
Titles
M.D., Ph.D
Expertise/Specialties
General Surgery, Gastrointestinal Surgery, Colorectal Surgery, Laparoscopic Surgery, Robotic Surgery, Minimally Invasive Surgery, Chemotherapy, Gastrointestinal Endoscopy, Colorectal Disease, Anorectal Disease, Colorectal Cancer, Inflammatory Bowel Disease, Diverticular Disease, Colorectal Polyp, Vascular Surgery, Abdominal Aortic Aneurysm, Thoracic Aortic Aneurysm, Endovascular Aneurysm Repair, Thoracic Endovascular Aortic Repair, Distal Bypass, Critical Limb Ischemia, Takayasu's Disease, Buerger Disease, Pancreatoduodeal Artery Aneurysm, Popliteal Entrapment Syndrome, Behçet's Disease, Carotid Endarterectomy, Hemodialysis, Peripheral Artery Aneurysm, Segmental Arterial Mediolysis, Deep Vein Thrombosis
Research Interests
Surgical Oncology, Vascular Surgery
Languages
Japanese/English
See More
Departments/Divisions
International Medical Center
University of Tokyo Tissue Bank
Artificial Organ and Transplantation Division, Department of Surgery
Titles
M.D., Ph.D., F.A.C.S.
Expertise/Specialties
Surgery, Heaptology, Liver Transplantation, Tissue Transplantation, Medical Education
Research Interests
Liver Disease, Liver Trasnplantation, Organ Transplantation, Donor Safety in Living Liver Donor, Tissue Transplantation, Tissue Banking, Cyropreservation of homograft, Medical Education, Surgical Training, Medical Care for Foreign Patients in Japan, Multicultural Resource for Health Care, Cross border clinical medicine
Languages
Japanese / English
See More
Departments/Divisions
Respiratory Medicine
Titles
M.D. , Ph.D.
Expertise/Specialties
Respiratory Medicine
Research Interests
The mechanism of respiratory diseases including COPD, asthma and pulmonary fibrosis
Languages
Japanese/English
See More
Departments/Divisions
University Hospital Medical Information Network Center Department of Heath Communication, School of Public Health, Faculty of Medicine, the University of Tokyo
Titles
M.D., Ph.D.
Expertise/Specialties
health communication, health informatics
Research Interests
Interpersonal and media-based health communication
Languages
Japanese/English
See More
Departments/Divisions
Department of Diabetes and Metabolic Diseases
Titles
M.D., Ph.D.
Expertise/Specialties
Diabetes, Metabolism, Obesity, Nutrition,
Research Interests
Pathogenesis of type2 diabetes, insulin resistance, adiponectin
Languages
Japanese / English
See More
Departments/Divisions
Clinical Research Support Center
Titles
M.D. , Ph.D.
Expertise/Specialties
Clinical Pharmacology, Neurology
Research Interests
Clinical Pharmacology, Neurology
Languages
Japanese, English
See More
Departments/Divisions
Otorhinolaryngology and Auditory and Voice Surgery
Titles
M.D. , Ph.D.
Expertise/Specialties
Otology, Audiology, Neurotology
Research Interests
Cochlear implant, hearing loss, regeneration, anti-aging
Languages
Japanese, English
See More
Departments/Divisions
Pathology
Titles
M.D. , Ph.D.
Expertise/Specialties
Gastrointestinal pathology
Research Interests
The pathology and molecular biology of gastrointestinal tumor
Languages
Japanese, English
See More
Departments/Divisions
Environment, Health and Safety Office
Titles
M.D., Ph.D.
Expertise/Specialties
Neurology
Research Interests
Clinical Neurology, Quality and Safety in Hospital Practice
Languages
Japanese, English
See More
Departments/Divisions
Obstetrics and Gynecology, Perinatal Center
Titles
M.D. , Ph.D.
Expertise/Specialties
Perinatal care for both normal and abnormal antepartum, labor, delivery, fetus and newborn, puerperium
Research Interests
Reproductive immunology / Perinatology / Reproductive Endocrinology
Languages
Japanese / English
See More
Departments/Divisions
Department of Diabetes and Metabolic Diseases
Titles
M.D. , Ph.D.
Expertise/Specialties
Internal Medicine, Diabetes, Metabolism, Nutrition, Obesity, Metabolic Syndrome, Diabetic Complications, Atherosclerosis, Insulin Resistance, Adipokines, Nuclear Receptors, Epigenetics, GWAS, Sportology, Anti-Aging Medicine
Research Interests
The mechanisms by which obesity results in insulin resistance, atherosclerosis and short life
Languages
Japanese / English
See More
Departments/Divisions
Stomach and Esophageal Surgery, Breast and Endocrine Surgery
Titles
M.D. , Ph.D.
Expertise/Specialties
Upper GI surgery, Esophageal Cancer, Gastric Cancer
Research Interests
surgical procedure and oncology of esophageal and gastric cancer
Languages
Japanese and English
See More
Departments/Divisions
Anesthesiology and Pain Relief Center
Titles
M.D. , Ph.D.
Expertise/Specialties
Anesthesiology, Critical care medicine, Respiratory care, Operative medicine, Pain medicine
Research Interests
Acute lung injury, Mechanical ventilation, acute inflammatory response, Mechanism of general anesthesia, Modulation of pain
Languages
Japanese/ English
See More
Departments/Divisions
Department of Child Psychiatry
Titles
M.D. , Ph.D.
Expertise/Specialties
Child and Adolescent Psychiatry, Tourette Syndrome and Other Tic Disorders, Obsessive-Compulsive Disorder (OCD), Attention-Deficit/Hyperactivity Disorder (ADHD), Autism Spectrum Disorder (ASD), School Mental Health
Research Interests
Phenomenology, Pathogenesis and Intervention of Tourette Syndrome and Comorbid Disorders Including OCD and ADHD
Languages
Japanese/English
See More
Departments/Divisions
Gynecologic Surgery
Titles
Professor
Expertise/Specialties
Reproductive medicine, laparoscopic surgery, assisted reproductive technology
Research Interests
Pathogenesis and management of endometriosis, Ovarian physiology/ pathology
Languages
Japanese / English
See More
Departments/Divisions
Department of Clinical Laboratory
Titles
M.D. , Ph.D.
Expertise/Specialties
Laboratory Medicine, Clinical Hematology, Thrombosis and Hemostasis
Research Interests
Platelet Biology, Vascular Biology, Bioactive Lipids
Languages
Japanese/ English
See More